humana consent form
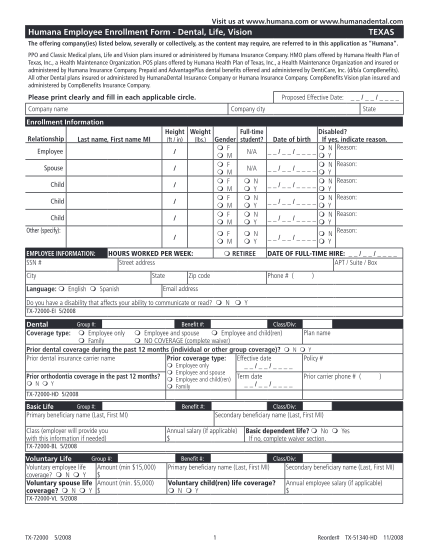
Your guide to ppo enrollment coveragefirst consent for release of protected health information member information (person whose information will be released): your name: date of birth: first middle last month day year address: street city state...
FILL NOW