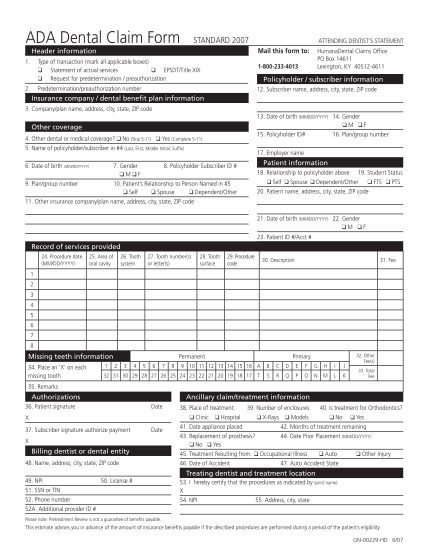
255-2301 SB.EE.10.OK 6 10. Health benefits claim form to be completed by the insured member for use with the Humana family of health insurance and health plan companies.
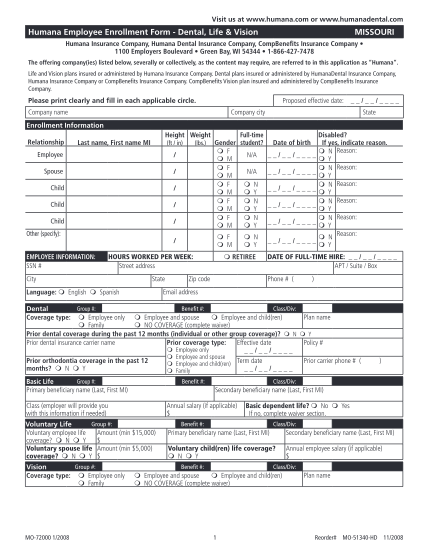
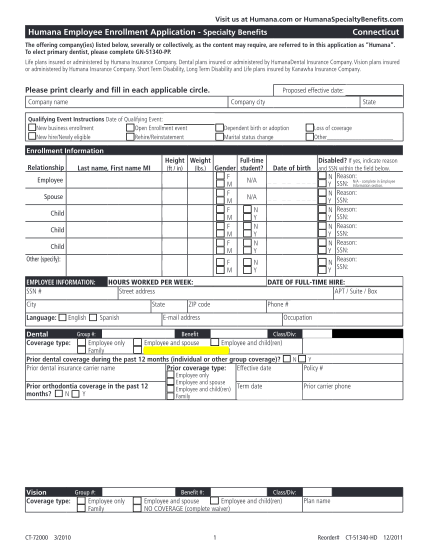
Print form group plan change request humana / humanadental we, us, and our refer to the insuring entities listed on the business profile section of the employer group application. agent/producer information (please provide your current...
FILL NOW