Adolescent/Adult Immunization Record - adph
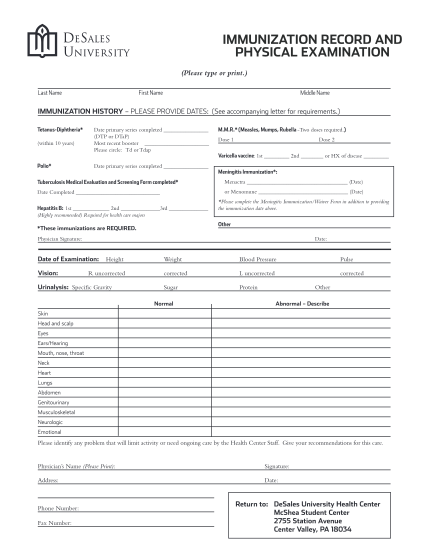
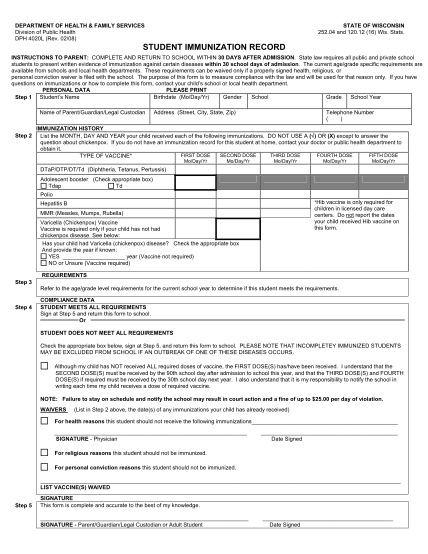
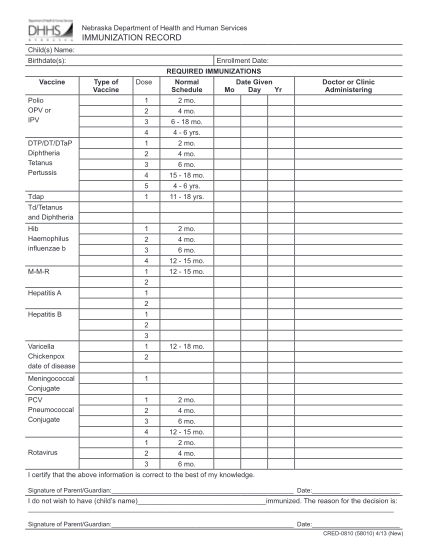
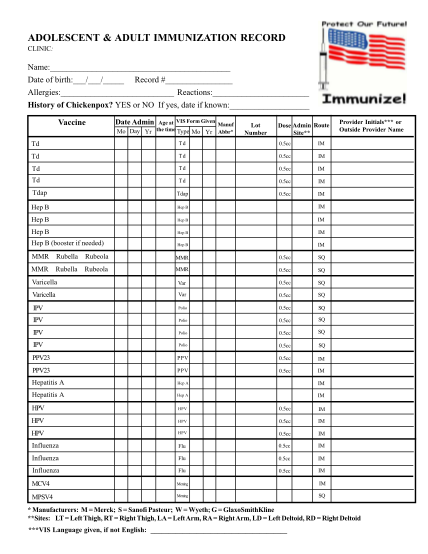
Adolescent & adult immunization record clinic: name: date of birth: / / record # allergies: reactions: history of chickenpox? yes or no if yes, date if known: vaccine age at vis form given manuf the time type mo mo day yr yr abbr* date admin lot...
FILL NOW