oxford health dom plan benefits form
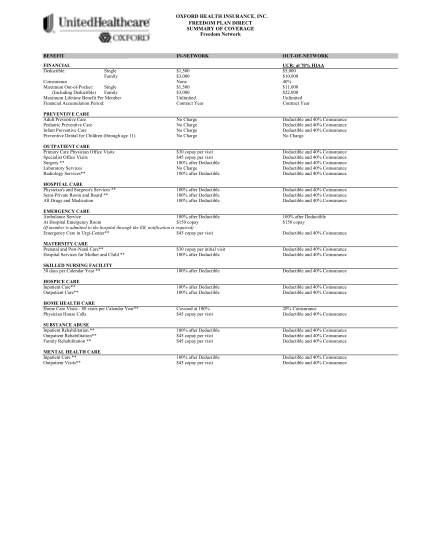
Oxford health insurance, inc. freedom plan direct summary of coverage freedom network benefit financial deductible: single family in-network $1,500 $3, none $1,500 $3, unlimited contract year no charge no charge no charge no charge $30 copay per...
FILL NOW