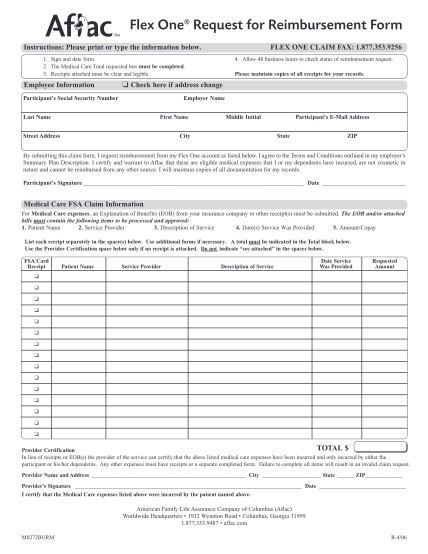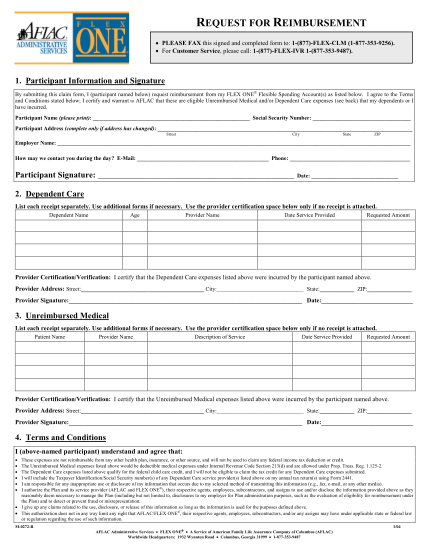
2010 Wellness Grant Request for Reimbursement Form - wcif
2010 wcif/wcip wellness grant program request for reimbursement form print form directions complete the following form to request reimbursement for wcif/wcip wellness grant funding. type is preferred wherever possible. 1. you must attach copies of...
FILL NOW