meritain provider appeal form
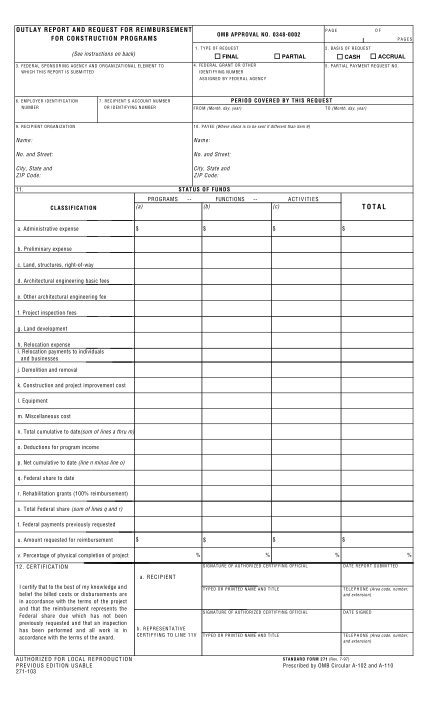
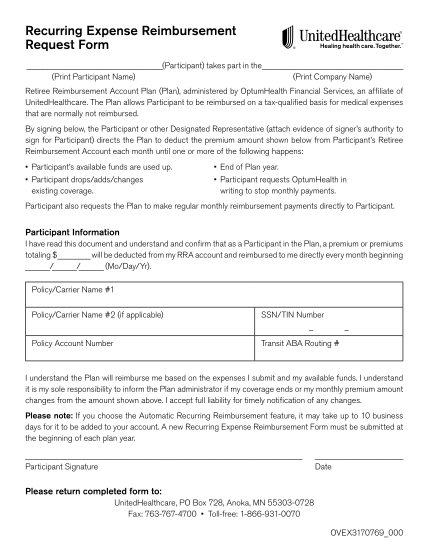
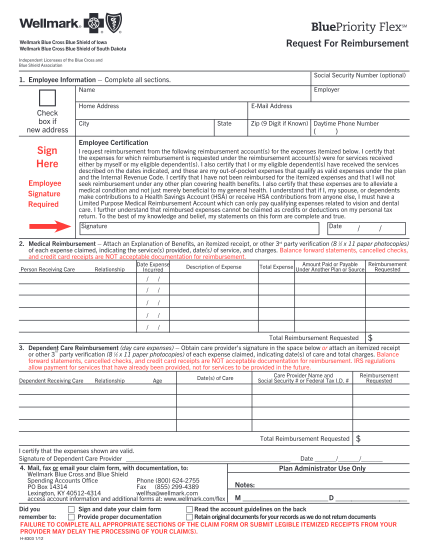
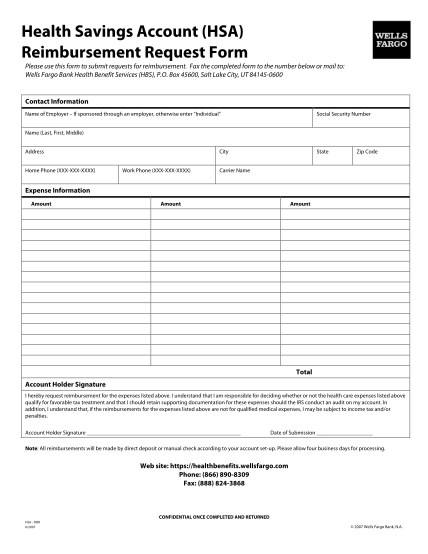
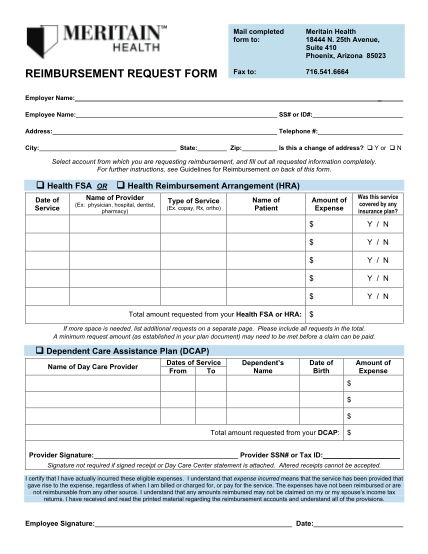
Reimbursement request form employer name: employee name: ss# or id#: address: telephone #: state: city: zip: is this a change of address? y or n select account from which you are requesting reimbursement, and fill out all requested information...
FILL NOW