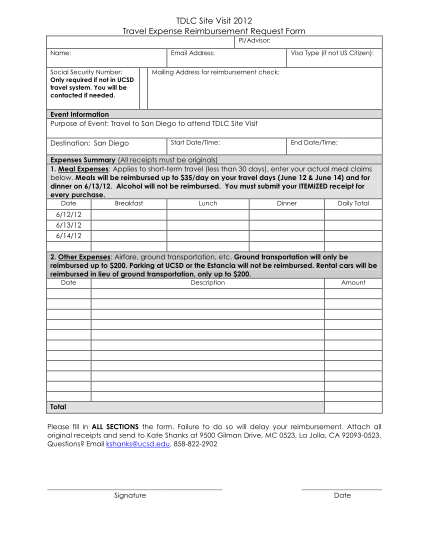
TDLC Site Visit 2012 Travel Expense Reimbursement Request Form - tdlc ucsd
Tdlc site visit 2012 travel expense reimbursement request form pi/advisor: name: social security number: only required if not in ucsd travel system. you will be contacted if needed. email address: mailing address for reimbursement check: visa type...
FILL NOW