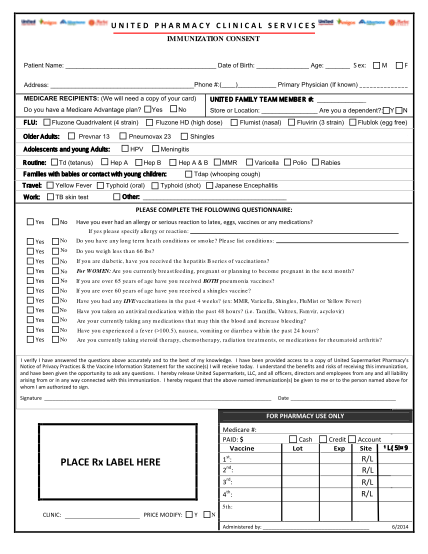
Immunization Consent Form - Albertsons Market
United pharmacy clinical services immunization consent patient name: date of birth: age: address: phone #:( ) primary physician (if known) medicare recipients: (we will need a copy of your card) do you have a medicare advantage plan? yes...
FILL NOW