hospital admission form
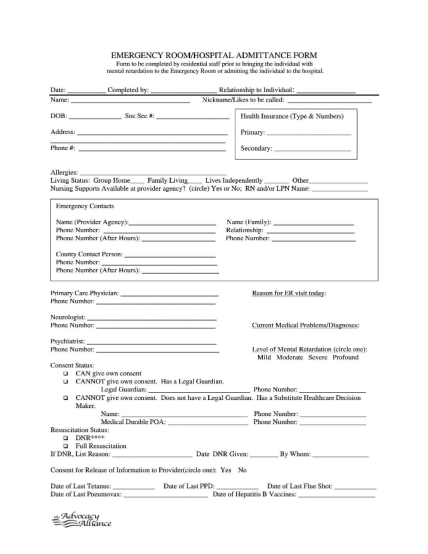
Patient admission form important: please send this completed form to the hospital where you will have your procedure/surgery. personal and administration details mr surname (family name): first name(s): date of birth: mrs ms miss mstr dr preferred...
FILL NOW