cardiac clearance doc
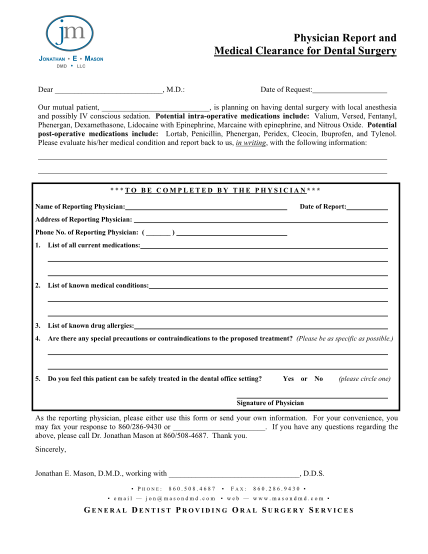
Cardiac clearance request date: / , 20 dear dr. cardiologist re: our mutual patient: dob: / / the patient is or will be, scheduled for surgery on , 20 requiring a mac or general anesthetic. length of procedure: hours minutes we are requesting...
FILL NOW