LETTER OF MEDICAL NECESSITY
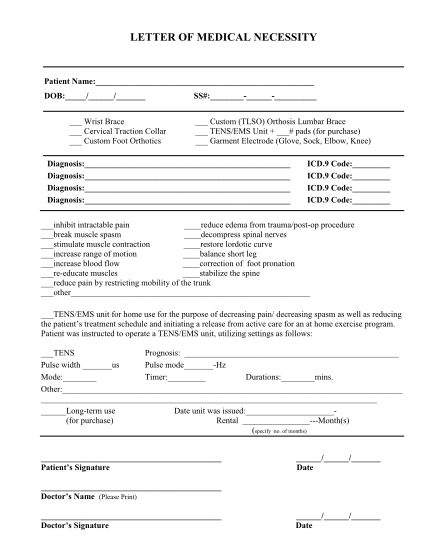
Letter of medical necessity patient name: dob: / / wrist brace cervical traction collar custom foot orthotics ss#: custom (tlso) orthosis lumbar brace tens/ems unit + # pads (for purchase) garment electrode (glove, sock, elbow, knee) diagnosis:...
FILL NOW