
psychiatric progress note template pdf
Outpatientioffice psychiatric progress note. counseling andior coordination of care. patient's name: date of visit: interval
FILL NOW Outpatientioffice psychiatric progress note. counseling andior coordination of care. patient's name: date of visit: interval
FILL NOW Outpatientioffice psychiatric progress note. counseling andior coordination of care. patient's name: date of visit: interval
FILL NOW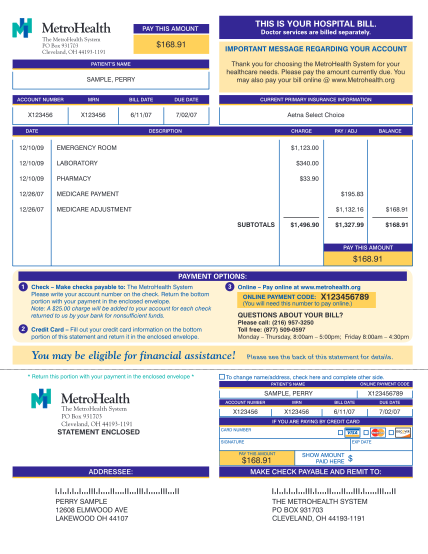
If paying by credit card, please fill out below make checks payable to: check card to be used for payment 9200 west wisconsin avenue milwaukee, wi 53226-3596 card number remit to: p.o. box 3202 milwaukee, wi 53201-3202 amount signature phone:...
FILL NOW If paying by credit card, please fill out below make checks payable to: check card to be used for payment 9200 west wisconsin avenue milwaukee, wi 53226-3596 card number remit to: p.o. box 3202 milwaukee, wi 53201-3202 amount signature phone:...
FILL NOW
Explanatory notewhen properly filled out, the following statement of defendant in support of guiltyplea contains all the requirements of rule 11(e), utah rules of criminal procedure. if thedistrict court chooses to rely on this statement for...
FILL NOW
The university of toledo -college of medicine excused absence pre-clinical years request form name: class year: address: city: state: zip: telephone: pager: beginning date: ending date: courses missed: reason for request: attach appropriate...
FILL NOW The university of toledo -college of medicine excused absence pre-clinical years request form name: class year: address: city: state: zip: telephone: pager: beginning date: ending date: courses missed: reason for request: attach appropriate...
FILL NOW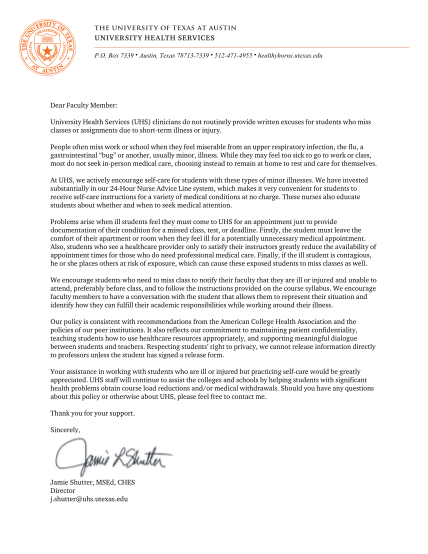
P.o. box 7339 austin, texas 78713-7339 512-471-4955 healthyhorns.utexas.edu dear faculty member: university health services (uhs) clinicians do not routinely provide written excuses for students who miss classes or assignments due to short-term...
FILL NOW
Patient registration form fields identified with an (*) must be completed. todays date: .. patient name (first, middle, last)*: date of birth*: / / ssn: gender: m male m female marital status: m single m married m divorced m widowed primary...
FILL NOW Patient registration form fields identified with an (*) must be completed. todays date: .. patient name (first, middle, last)*: date of birth*: / / ssn: gender: m male m female marital status: m single m married m divorced m widowed primary...
FILL NOW
For internal purposes account number: medical record number: health system authorization for the release of protected health information social security number (last 4 digits only): patient name: previous name, if applicable: address: city: date...
FILL NOW For internal purposes account number: medical record number: health system authorization for the release of protected health information social security number (last 4 digits only): patient name: previous name, if applicable: address: city: date...
FILL NOW