101530-14 - Medical
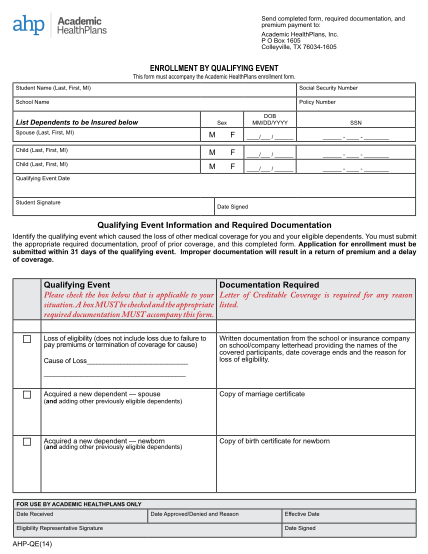
Academic healthplans send completed form, required documentation, and premium payment to: academic healthplans, inc. p o box 1605 colleyville, tx 760341605 enrollment by qualifying event this form must accompany the academic healthplans enrollment...
FILL NOW