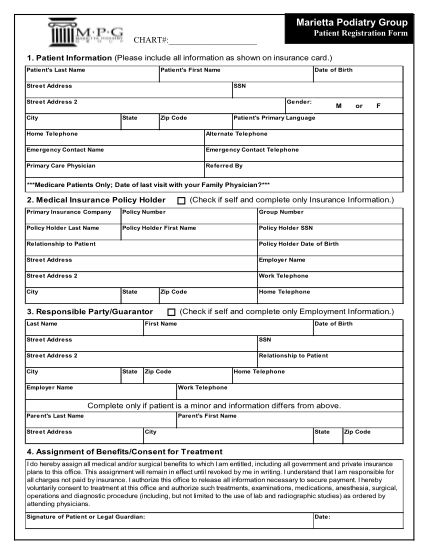
) Patie nt 's Last Name Patient 's First Name Stre et Address Date of Birth SSN Ge nder: Stre et Address 2 City State Zip Code M or F Patient 's Primary Language Home Telephone Alternate Te lephone Emerge ncy Contact Name Emerge ncy Contact
Marietta podiatry group patient registration form chart#: 1. patient information (please include all information as shown on insurance card.) patie nt 's last name patient 's first name stre et address date of birth ssn ge nder: stre et address 2...
FILL NOW