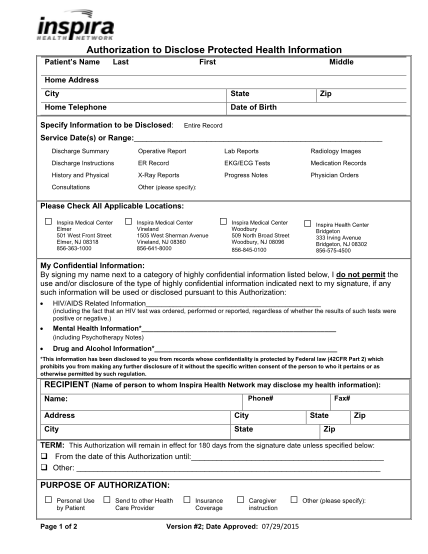
Hospital Medical Record Request Form - Inspira Health Network - inspirahealthnetwork
Authorization to disclose protected health information patients name last first middle home address city state home telephone date of birth specify information to be disclosed: zip entire record service date(s) or range: discharge summary...
FILL NOW