bcbs ohio prior authorization form
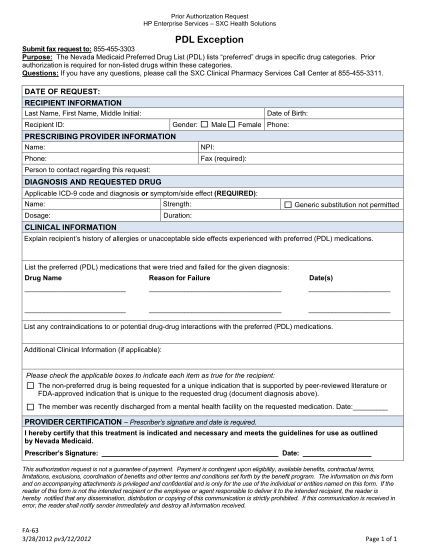
Prior authorization request hp enterprise services ? sxc health solutions ? pdl exception submit fax request to: 855-455-3303 purpose: the nevada medicaid preferred drug list (pdl) lists ?preferred? drugs in specific drug categories. prior...
FILL NOW