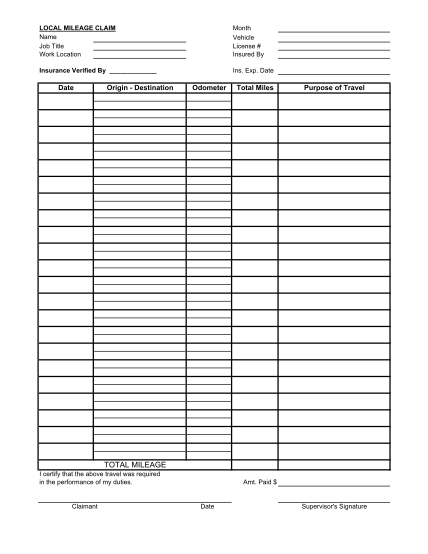
Workers comp mileage form - Submit your mileage for all trips that exceed 5 miles round trip, if the purpose of
Workers' compensation request for mileage reimbursement claim number: employer: date of accident: claimant: date of trip c22733 4/04 address from destination attention: parking/tolls (receipt must be included) number of miles round
FILL NOW