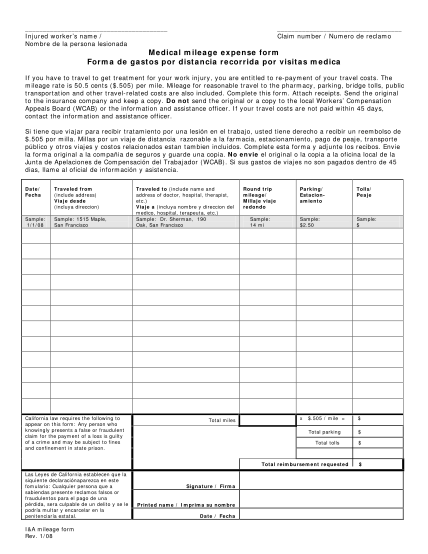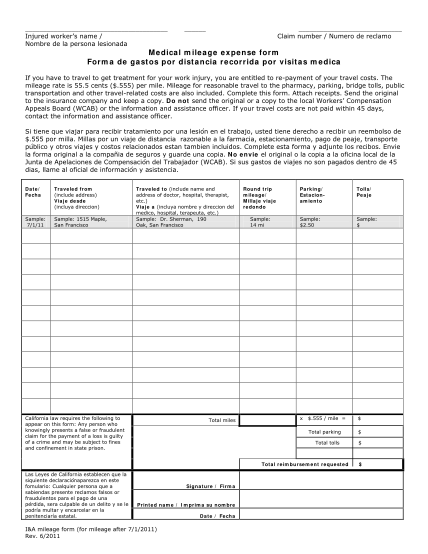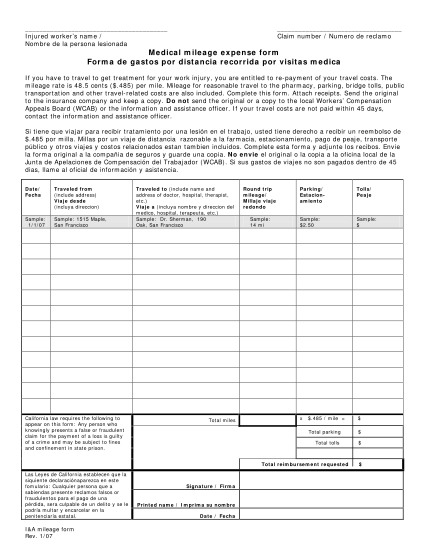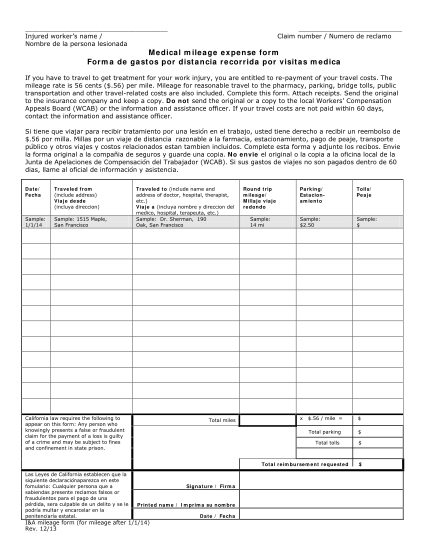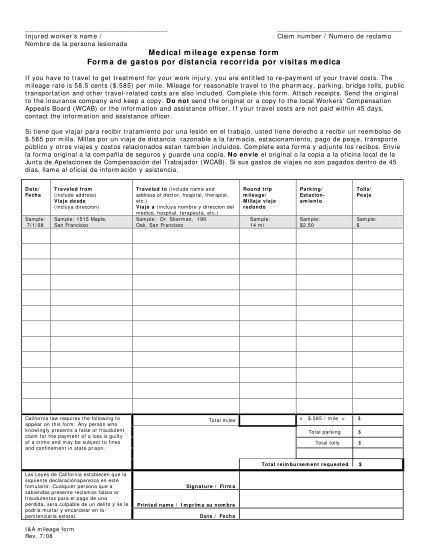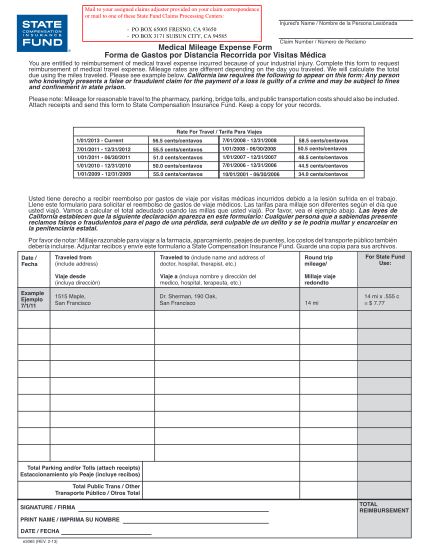
BESTflex Plan Medical Mileage Expense Form
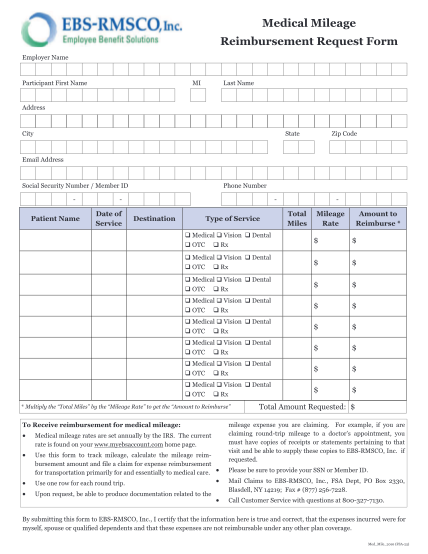
Orthodontic care expense receipt (must submit with completed claim form) fax to: mail to: phone support: e-mail support: section 125 administration 608 831 4790 employee benefits corporation, po box 44347, madison wi 53744-4347 800 346 2126, 608...
FILL NOW