en Insiders Guide to Mobile Free Edition Pre Release Version - PDF ...
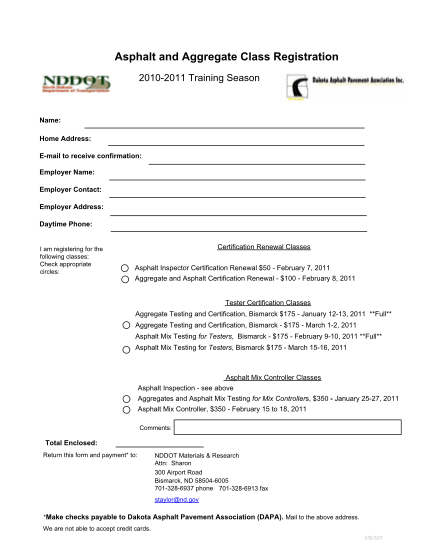
Click here to print this for asphalt and aggregate class registration 2010-2011 training season name: tex te t home address: e-mail to receive confirmation: employer name: employer contact: employer address: daytime phone: i am registering for the...
FILL NOW