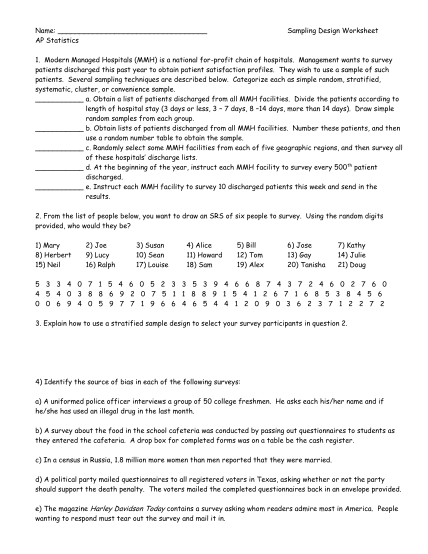
NEW PATIENT bHEALTH QUESTIONNAIREb bb - StudentZone - studentzone roehampton ac
New patient health questionnaire welcome to the student medical centre to help us with your past medical history we wold be grateful if you would complete this questionnaire along with anything else you feel we should know all information is...
FILL NOW