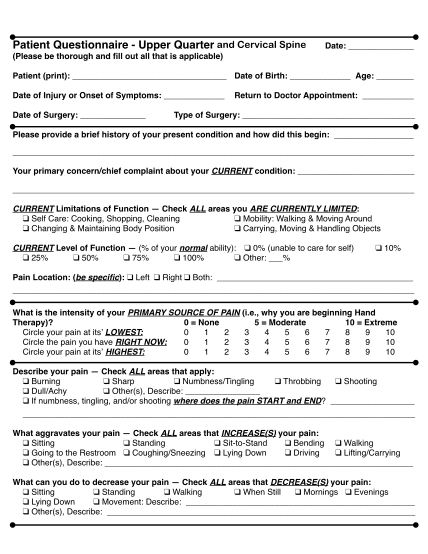
Patient Questionnaire - Hospital for Special Surgery - hss
Welcome to the office of dr. peter j. moley patient questionnaire: name: date of service: dominant hand: right left gender: male female date of birth: referred by: doctor: patient: chief complaint: onset of symptoms:
FILL NOW