universal medication form printable
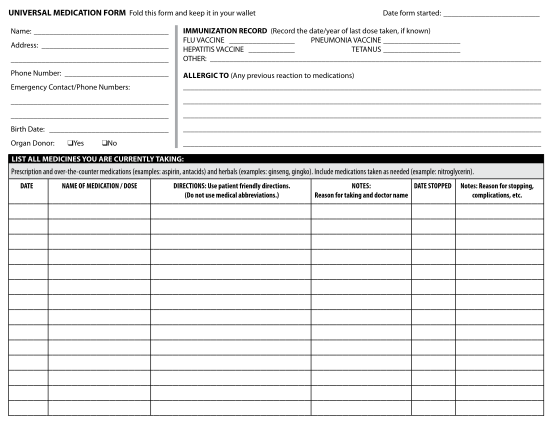
Universal medication form fold this form and keep it in your wallet name: phone number: birth date: emergency contact/phone numbers: date form started: address: medical record #: immunization record (record the date/year of last dose taken, if...
FILL NOW