affordable dentures new patient forms
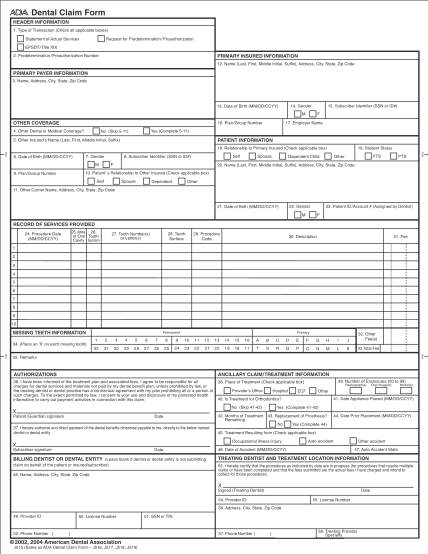
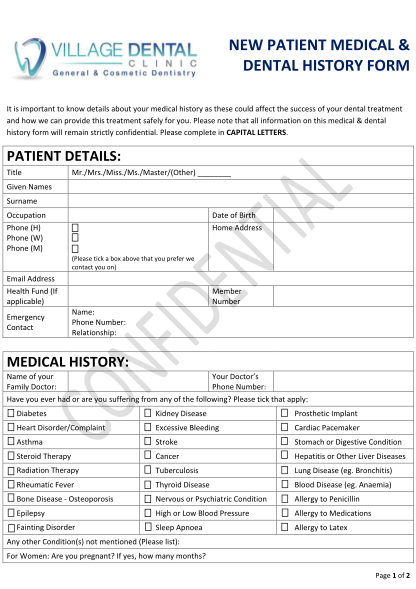
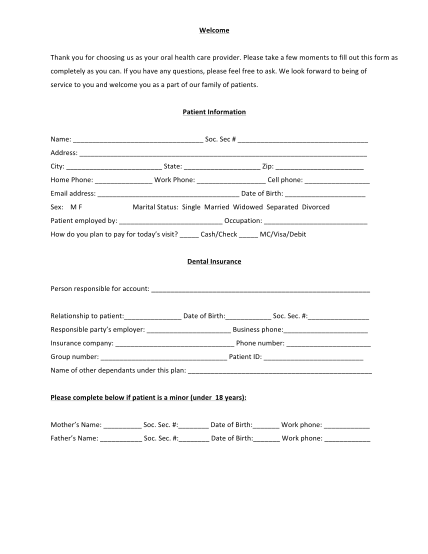
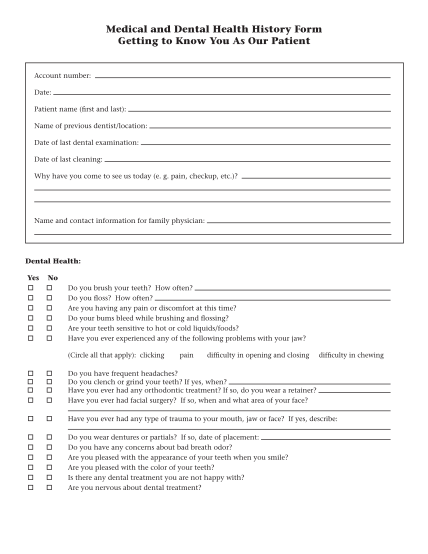
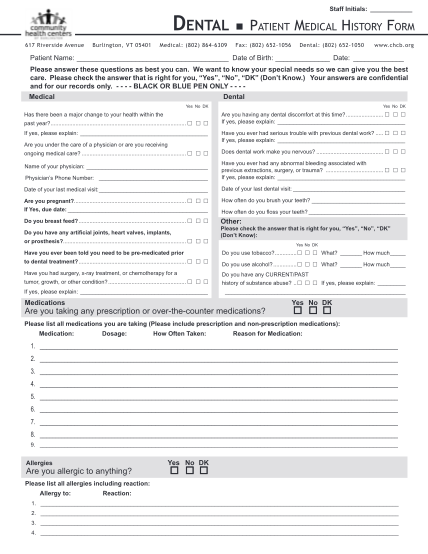
An affiliated practice providing patient history information patient id # for office use: name: (last name) (first name) (middle name) sex: m f date of birth: / / social security number: - - street address: city: state: zip: e-mail: home phone:...
FILL NOW