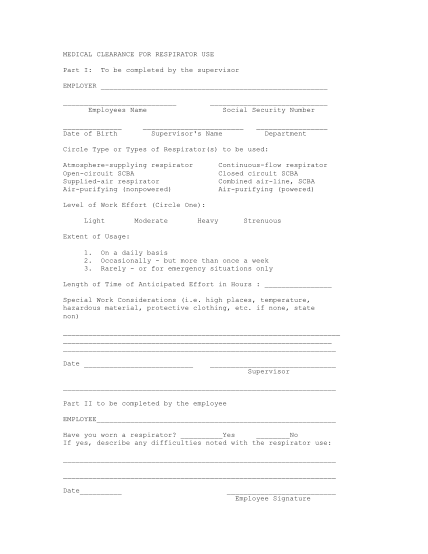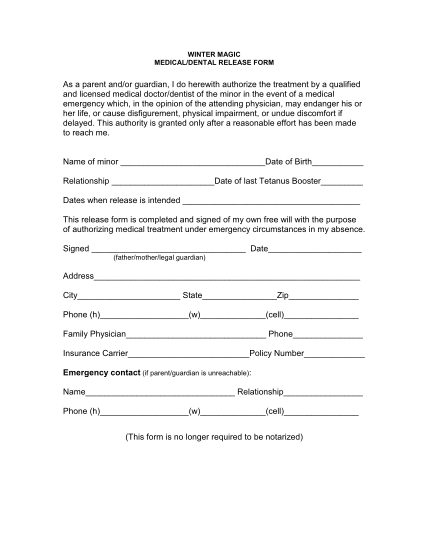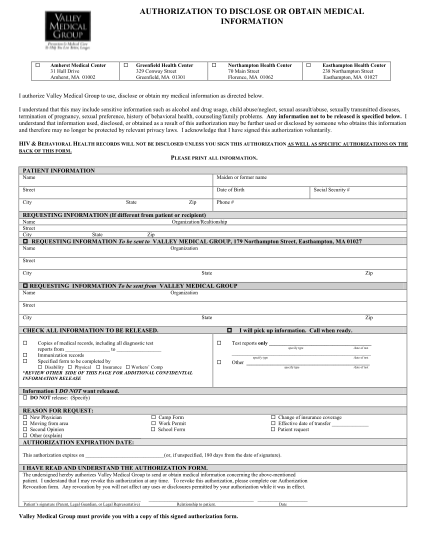
printable surgical clearance form
Medical clearance form for participation in physical exercise program please print: patient: date: address: telephone:( ) birth date: sex: 1. physical examination: a. b. blood pressure (sitting) ra la c. resting heart rate bpm d. 2. height inches...
FILL NOW