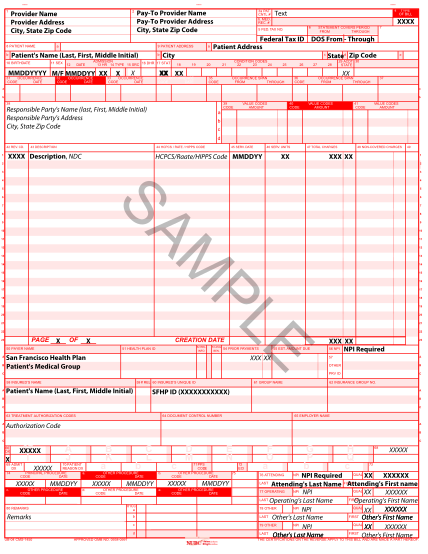
fdb claim form
United states district court ? district of massachusetts if you are a consumer or third-party payor that paid for all or part of the cost of prescription drugs based in any part on price information reported by first databank, inc., a proposed...
FILL NOW