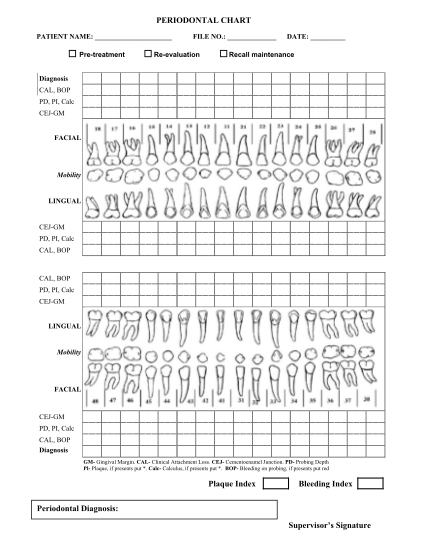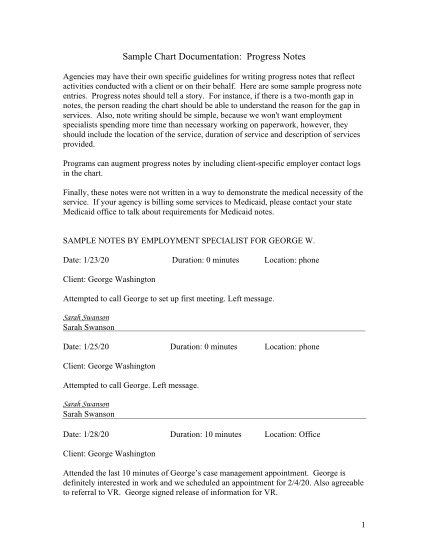
patient chart pdf
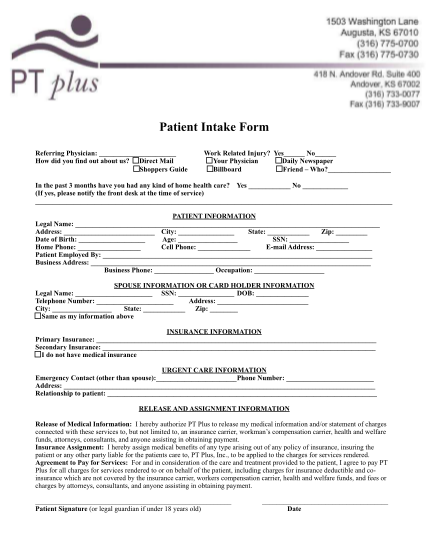
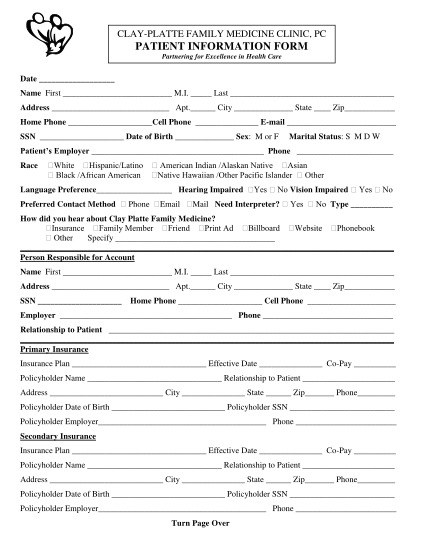
Clay-platte family medicine clinic, pc patient information form partnering for excellence in health care date name first m.i. last address apt. city state zip home phone cell phone e-mail ssn date of birth sex: m or f marital status: s m d w...
FILL NOW