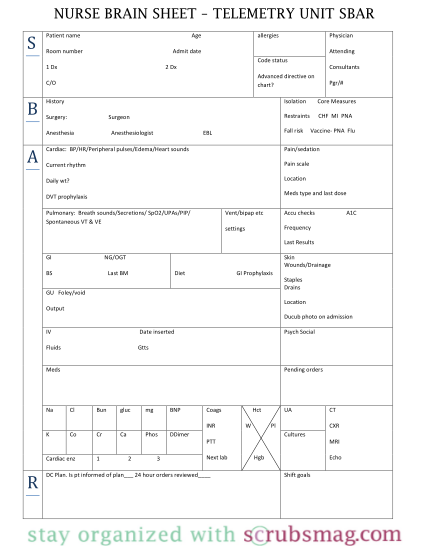
sbar chart template
Sbar hand-off form. sbar report form. form 322-1015 11/09. s ( situation). diagnosis: code: d full d partial d dnr d palliative
FILL NOW Sbar hand-off form. sbar report form. form 322-1015 11/09. s ( situation). diagnosis: code: d full d partial d dnr d palliative
FILL NOW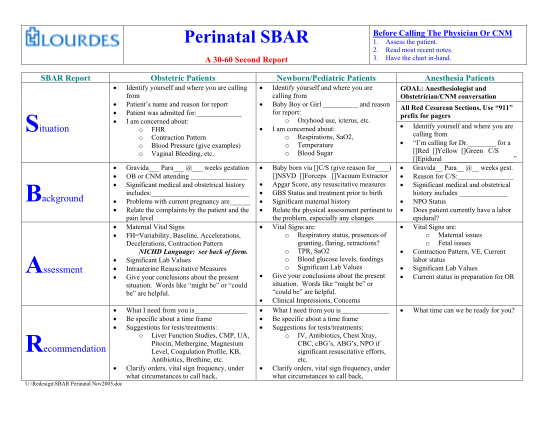
Perinatal sbar a 30-60 second report sbar report before calling the physician or cnm 1. 2. 3. assess the patient. read most recent notes. have the chart in-hand. obstetric patients identify yourself and where you are calling from patient's name...
FILL NOW Perinatal sbar a 30-60 second report sbar report before calling the physician or cnm 1. 2. 3. assess the patient. read most recent notes. have the chart in-hand. obstetric patients identify yourself and where you are calling from patient's name...
FILL NOW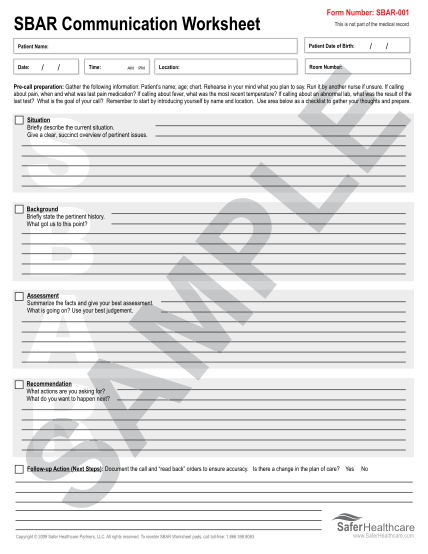
S sbar report to clinician about a clinical obstetric situation situation i am calling about (woman s name): ward: hosp no: the problem i am calling about is: i have just made an assessment: the vital signs are: blood pressure / pulse respirations...
FILL NOW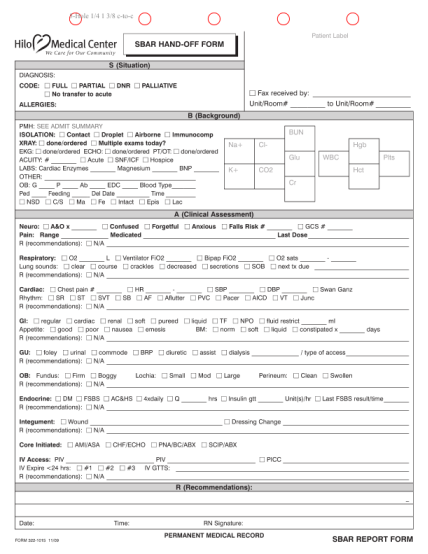
Sbar communication worksheet / this is not part of the medical record / patient date of birth: patient name: date: form number: sbar-001 / time: am pm location: / room number: pre-call call preparation: gather the following information: patient s...
FILL NOW Sbar communication worksheet / this is not part of the medical record / patient date of birth: patient name: date: form number: sbar-001 / time: am pm location: / room number: pre-call call preparation: gather the following information: patient s...
FILL NOW
Request for level ii pasrr evaluation and determination or resident review section i: request information date: request for: initial level ii evaluation and determination or resident review from: agency: phone: to: agency: phone: an indication of,...
FILL NOW
Piedmont community services form #128 rev. 1/6/2004 vital sign flow sheet height date weight attending physician pulse initial temperature first blood pressure last name b/p t p wt h signature / comments birthdate client
FILL NOW Piedmont community services form #128 rev. 1/6/2004 vital sign flow sheet height date weight attending physician pulse initial temperature first blood pressure last name b/p t p wt h signature / comments birthdate client
FILL NOW