2014 06 21 KAB PT Assessment Form- GENERAL
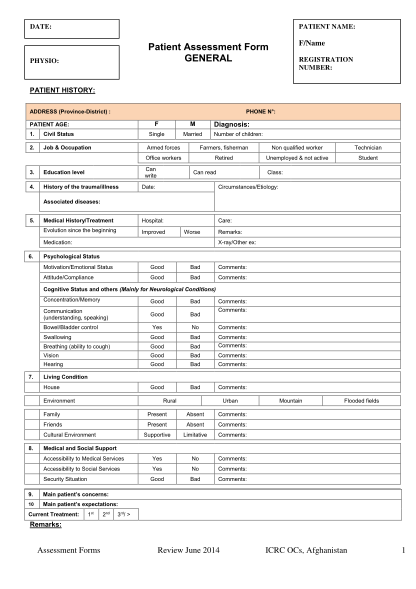
Date: patient name: f/name patient assessment form general physio: registration number: patient history: address (provincedistrict) : phone n: f 1. civil status 2. job & occupation m single patient age: married diagnosis: number of children: armed...
FILL NOW