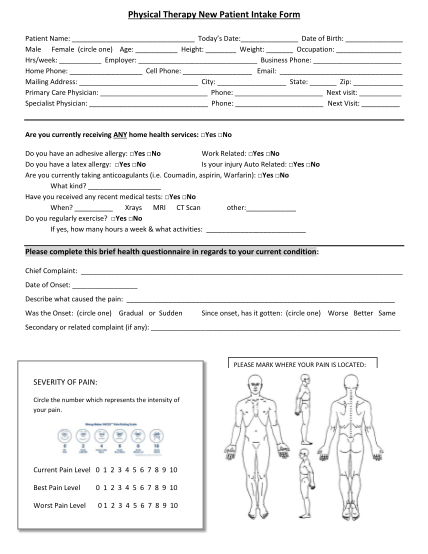
Patient sign in sheet template - therapy intake form
Patient intake form referring physician: how did you find out about us? direct mail shoppers guide work related injury? yes no your physician daily newspaper billboard friend who? in the past 3 months have you had any kind of home health care? yes...
FILL NOW