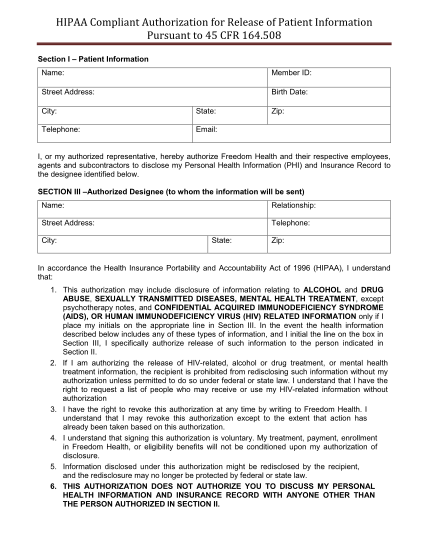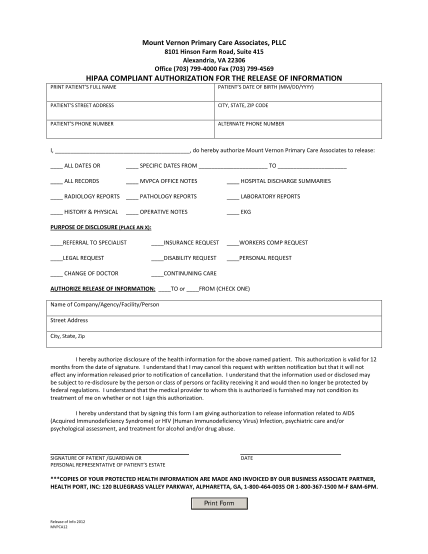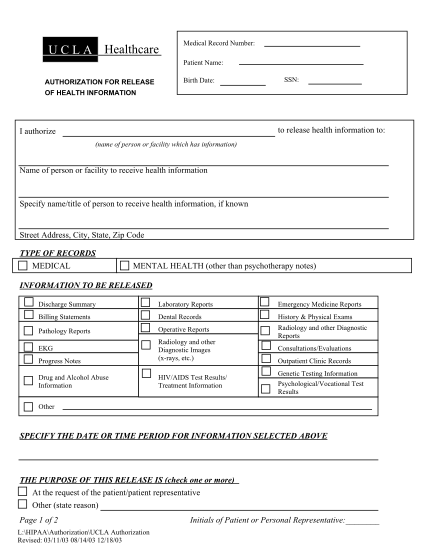
HIPAA COMPLIANT AUTHORIZATION FOR RELEASE OF HEALTH INFORMATION revised.doc. Records Request Form
Hipaa compliant authorization for release of health information patient name: date of birth: previous name/s (aka): social security number: i authorize: name of designated individual, organization, or provider address to release my health care...
FILL NOW