50311E1 Search and Seizure Documentation Administrators Form and Guide
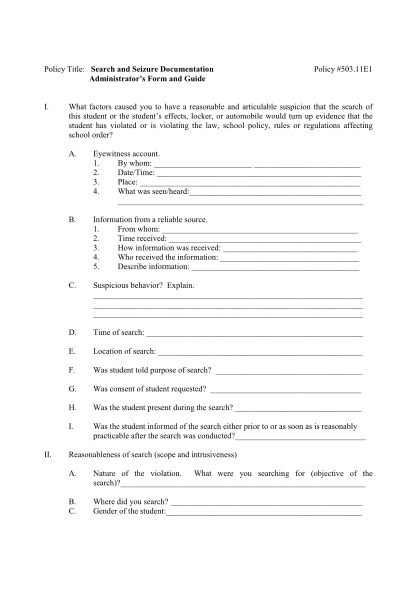
Policy title: search and seizure documentation administrators form and guide i. policy #503.11e1 what factors caused you to have a reasonable and articulable suspicion that the search of this student or the students effects, locker, or automobile...
FILL NOW