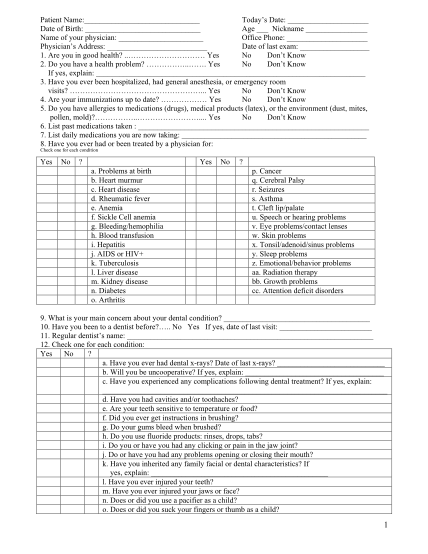
Patient Name: Todays Date: Date of Birth: Age Nickname Name of your physician: Office Phone: Physicians Address: Date of last exam: 1
Patient name: todays date: date of birth: age nickname name of your physician: office phone: physicians address: date of last exam: 1. are you in good health? .. yes no dont know 2. do you have a health problem? yes no dont know if yes, explain:...
FILL NOW