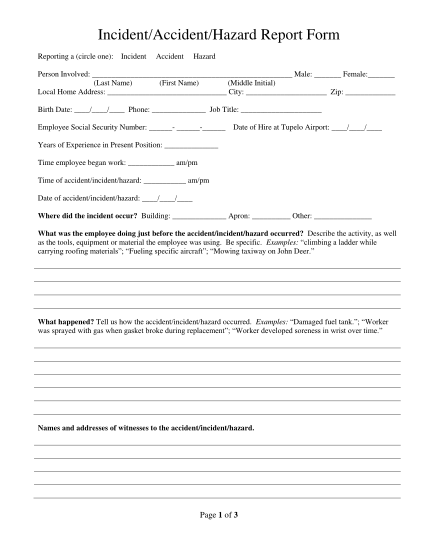
Accident and Injury Report & Form 19 - Hertford County - hertfordcountync
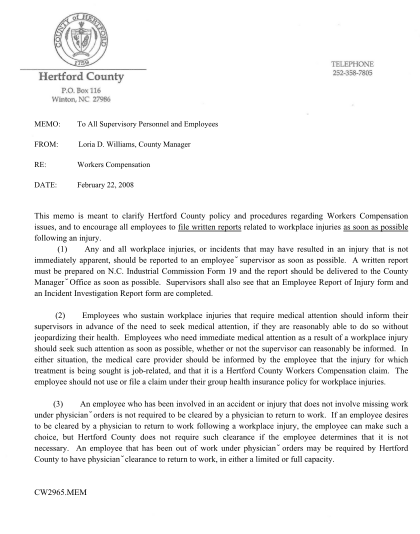
Memo: to all supervisory personnel and employees from: loria d. williams, county manager re: workers compensation date: february 22, 2008 this memo is meant to clarify hertford county policy and procedures regarding workers compensation issues,...
FILL NOW