2013 NSHE Foreign Workers Compensation Insurance Poster - bcn-nshe
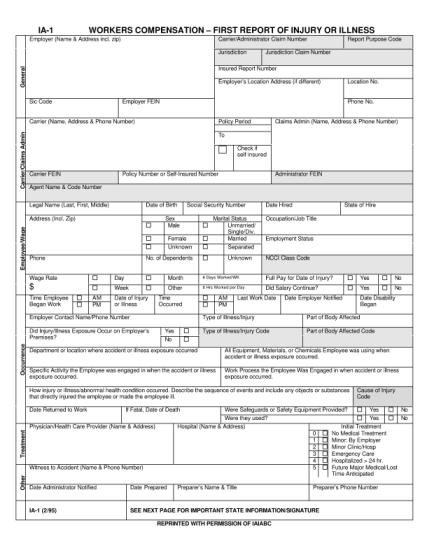
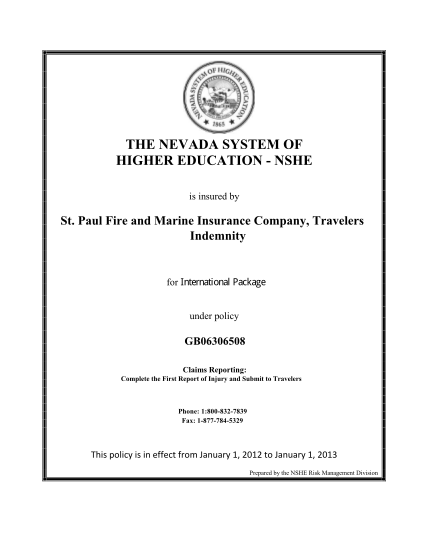
The nevada system of higher education - nshe is insured by st. paul fire and marine insurance company, travelers indemnity for under policy gb06306508 claims reporting: complete the first report of injury and submit to travelers phone:...
FILL NOW