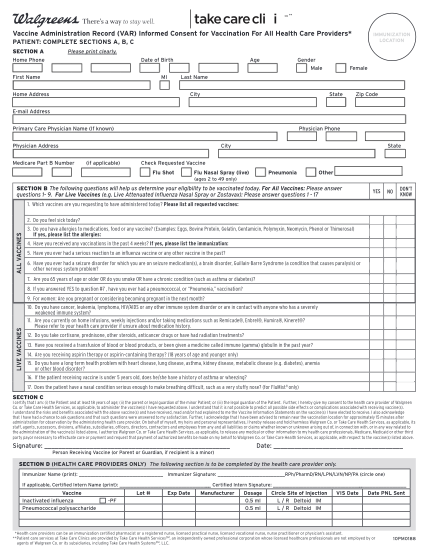
(VAR) Informed Consent for Vaccination For - City of Columbia ...
** vaccine administration record (var) informed consent for vaccination for all health care providers* immunization location patient: complete sections a, b, c section a please print clearly. home phone date of birth first name mi age gender male...
FILL NOW