preauthorazation from appolo munch
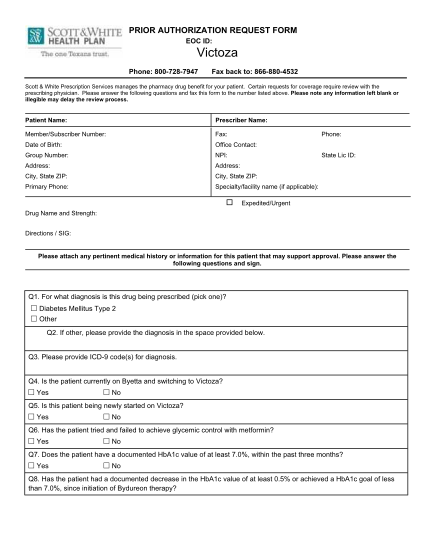
Prior authorization request form eoc id: phone: 800-728-7947 fax back to: 866-880-4532 scott & white prescription services manages the pharmacy drug benefit for your patient. certain requests for coverage require review with the prescribing...
FILL NOW