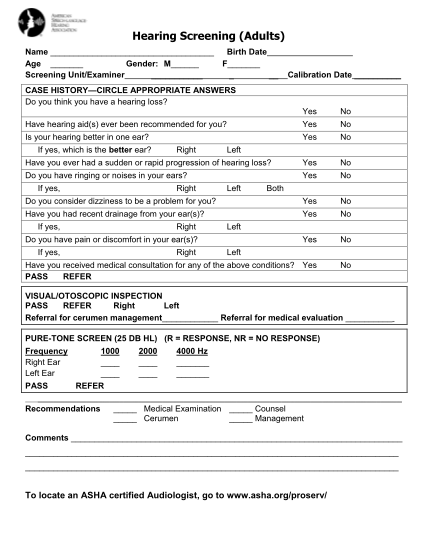
hearing screening form
Hearing screening (adults) name birth date age gender: m f screening unit/examiner calibration date case history circle appropriate answers do you think you have a hearing loss? yes no have hearing aid(s) ever been recommended for you? yes no is...
FILL NOW