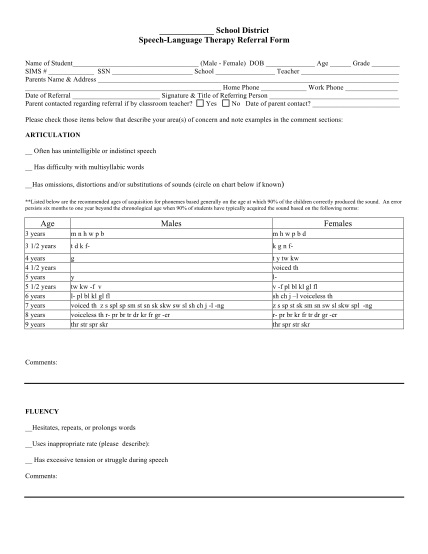
School District Speech-Language Therapy Referral Form - mitchell k12 sd
School district speechlanguage therapy referral form name of student (male female) dob age grade sims # ssn school teacher parents name & address home phone work phone date of referral signature & title of referring person parent contacted...
FILL NOW