general release of information form pdf
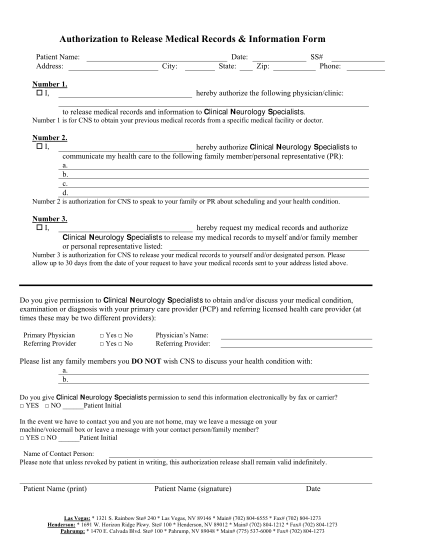
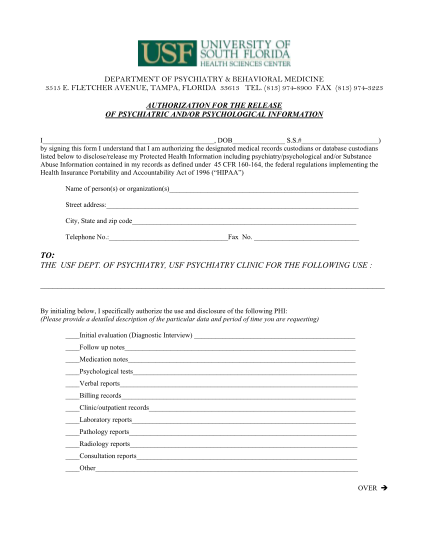
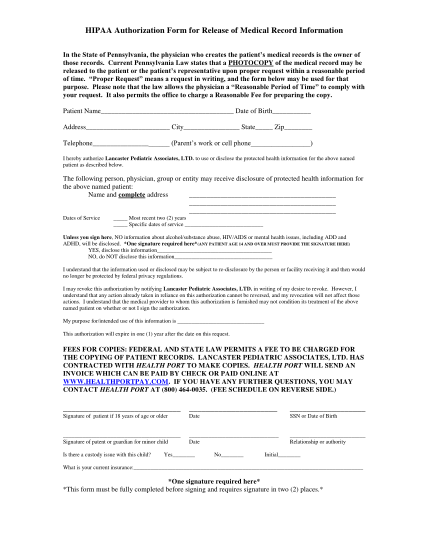
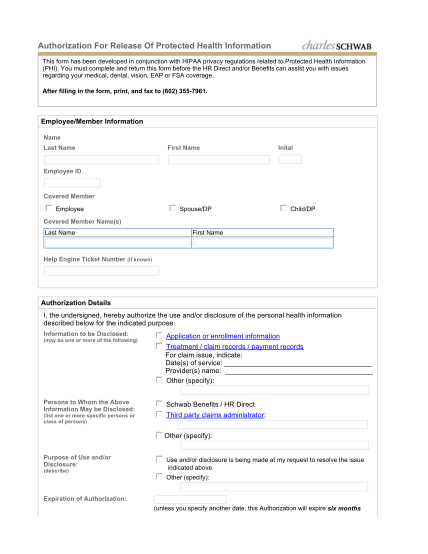
Denton heart group authorization to release medical records name of patient date of birth date(s) of service social security number i, the undersigned, authorize the release of, or request access to the information specified below from the medical...
FILL NOW