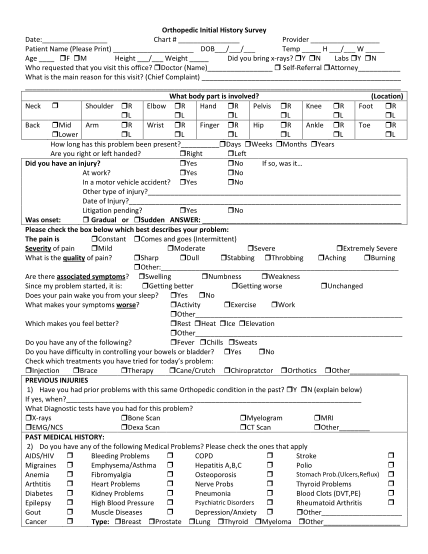
Orthopedic Initial History Survey Date: Chart # Provider Patient ...
Orthopedic initial history survey date: chart # provider patient name (please print) dob / / temp h / w age f m height / weight did you bring xrays? y n labs y n who requested that you visit this office? doctor (name) selfreferral attorney what is...
FILL NOW