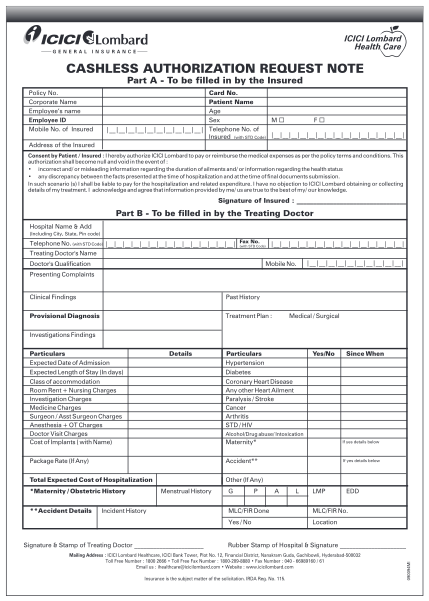
090094MI PRE AUTHORIZATION FORM ONE PAGE
Icici lombard health care cashless authorization request note part a - to be filled in by the insured policy no. corporate name employee s name employee id mobile no. of insured card no. patient name age sex m f telephone no. of insured (with std...
FILL NOW