1 04
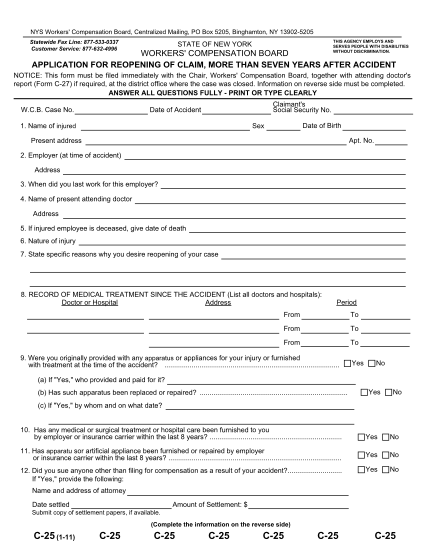
State of new york workers' compensation board this agency employs and serves people with disabilities without discrimination. notice of election of a not-for-profit corporation or a not-for-profit unincorporated association to exclude an...
FILL NOW