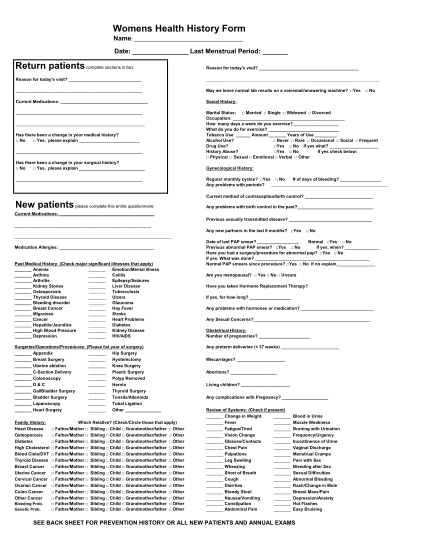
Womens Health History Form - Intermountain Healthcare - intermountainhealthcare
Womens health history form name: date: last menstrual period: return patients complete sections in box: reason for today's visit? current medications: has there been a change in your medical history? no yes, please explain has there been a change...
FILL NOW