Mileage Reimbursement Form - Blue Cross and Blue Shield of ... - bcbsal
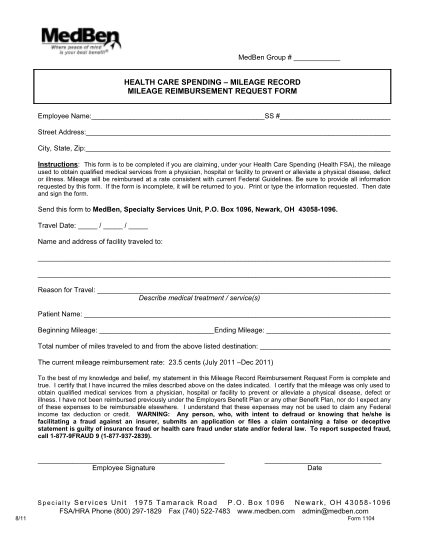
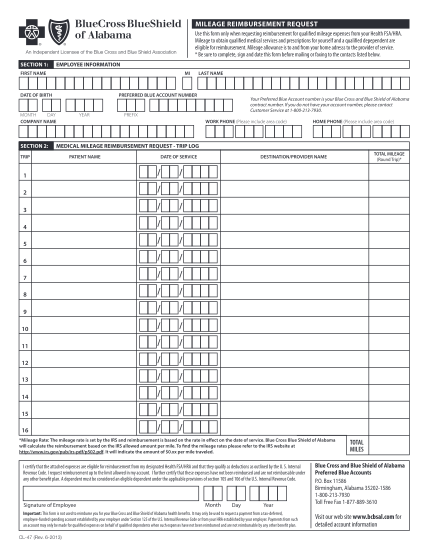
Mileage reimbursement request use this form only when requesting reimbursement for qualified mileage expenses from your health fsa/hra. mileage to obtain qualified medical services and prescriptions for yourself and a qualified depependent are...
FILL NOW