nike claim form
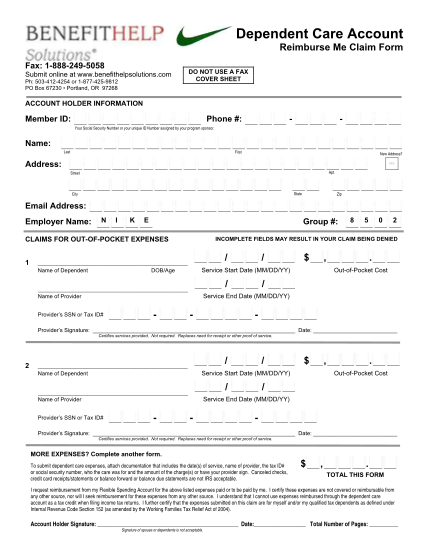
Dependent care account reimburse me claim form fax: 1--249-5058 submit online at .benefithelpsolutions.com ph: 503-412-4254 or 1-877-425-9812 po box 67230 portland, or 97268 do not use a fax cover sheet account holder information member id: phone...
FILL NOW