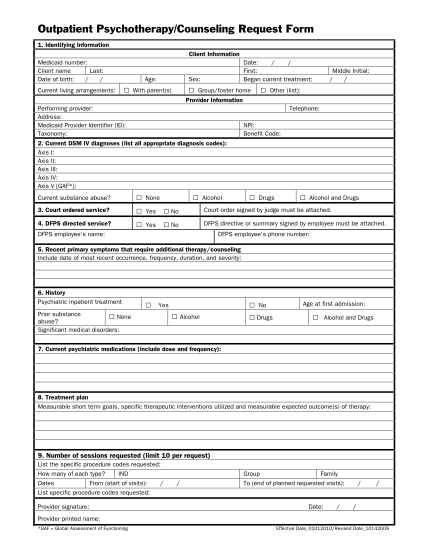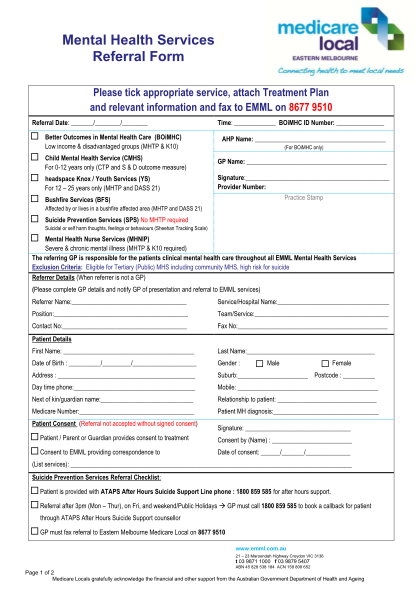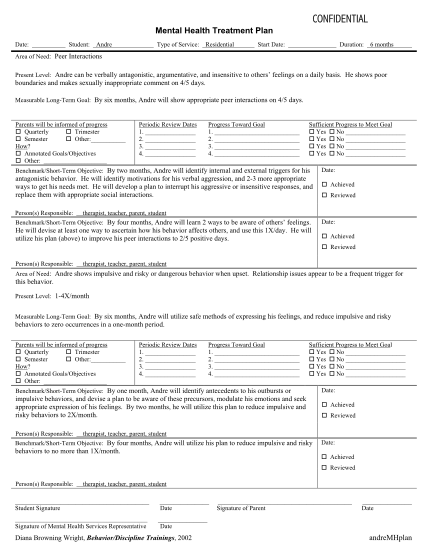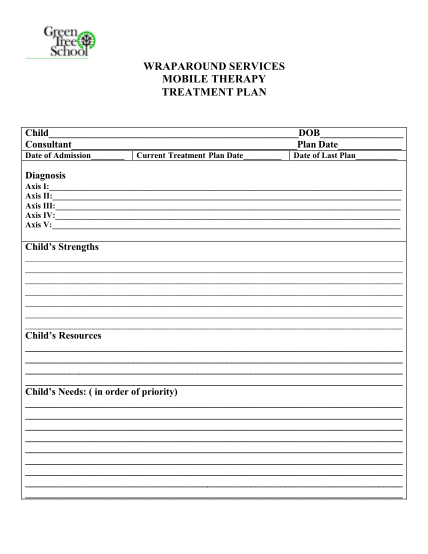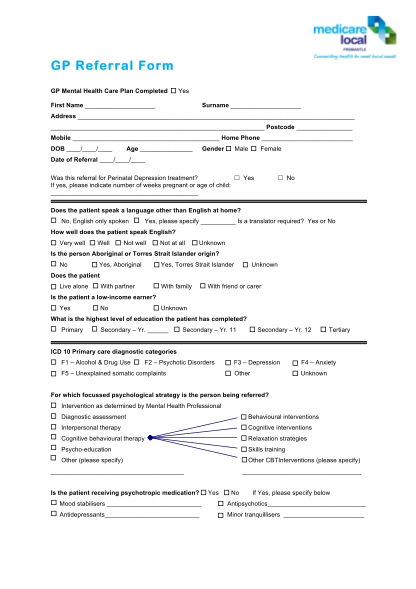
Treatment plan template - delta care referral form
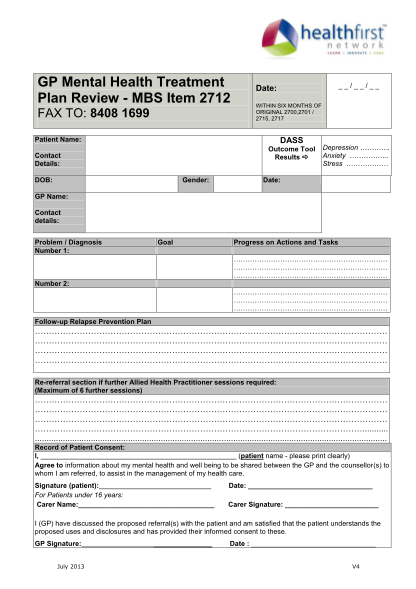
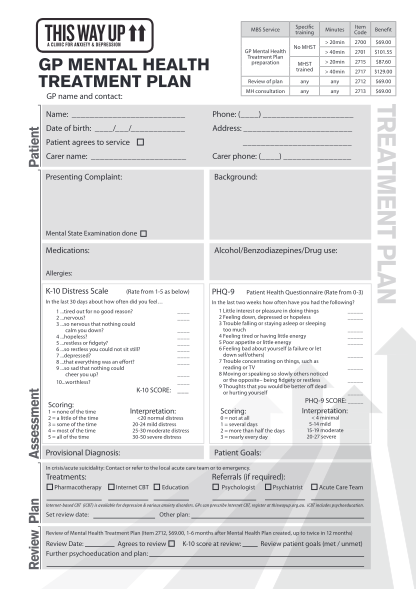
Stc1 mental health treatment plan patient identification multidisciplinary treatment plan development g 72 hour mtp development g subsequent review date: time: treatment plan reviewed and/or revised as below g social assessment performed: (see...
FILL NOW