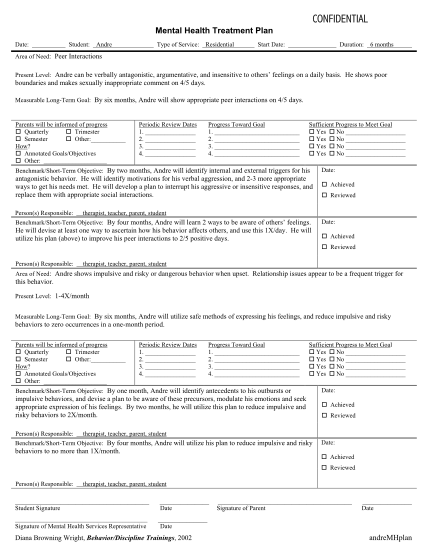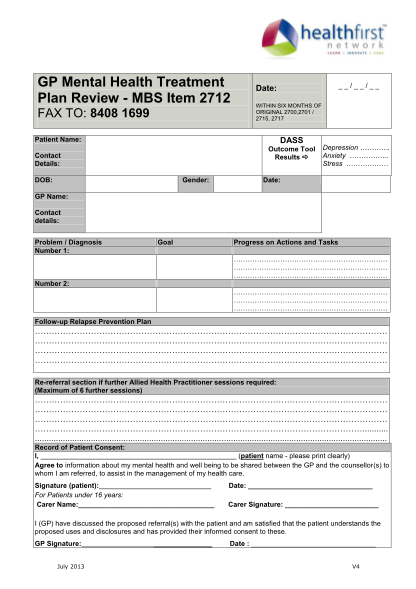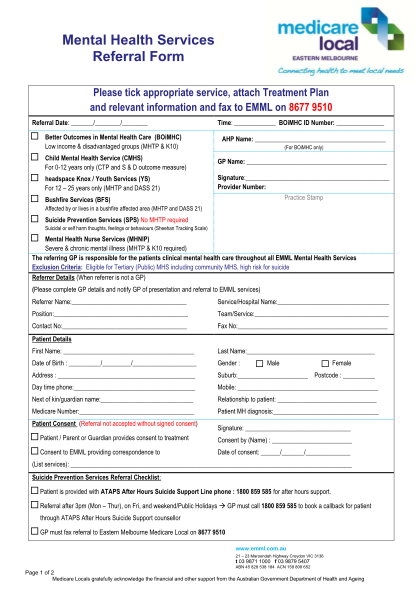
Treatment plan template mental health - mental health treatment plan
Please fax to: (812) 3787054 outpatient mental health treatment plan patients date of birth: member id number: precert #: physicians name facility: patients id number date of initial evaluation: frequency of therapy: expected length of treatment:...
FILL NOW