Capricornia Bushwalkers Inc Membership Application I - cbw bwq org
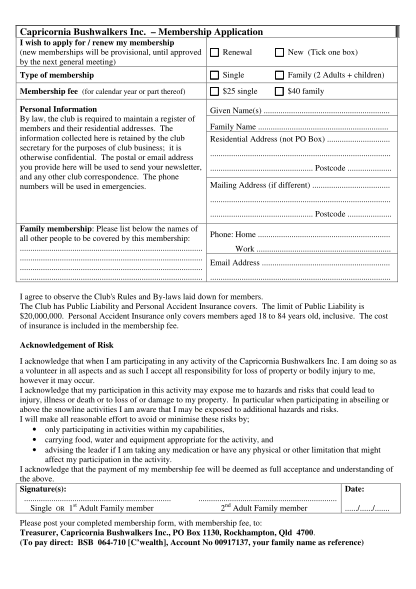
Capricornia bushwalkers inc. membership application i wish to apply for / renew my membership (new memberships will be provisional, until approved by the next general meeting) renewal new (tick one box) type of membership single family (2 adults +...
FILL NOW