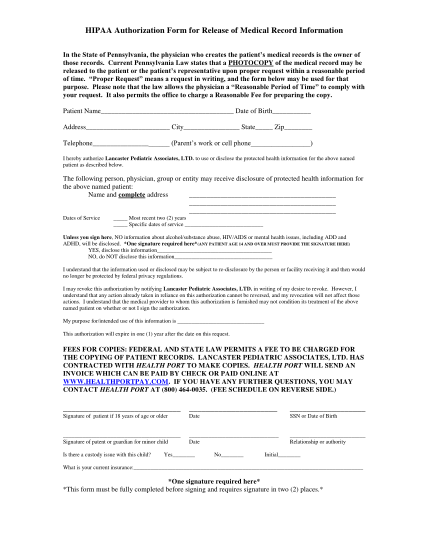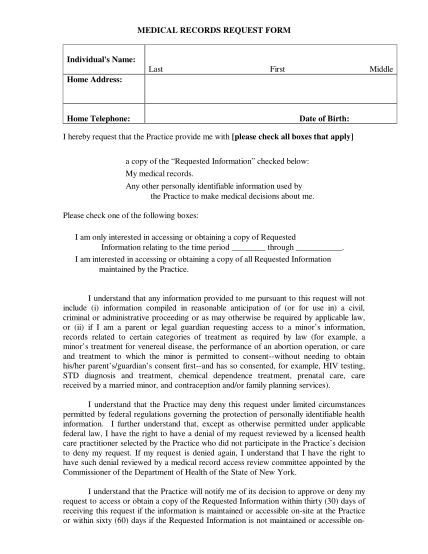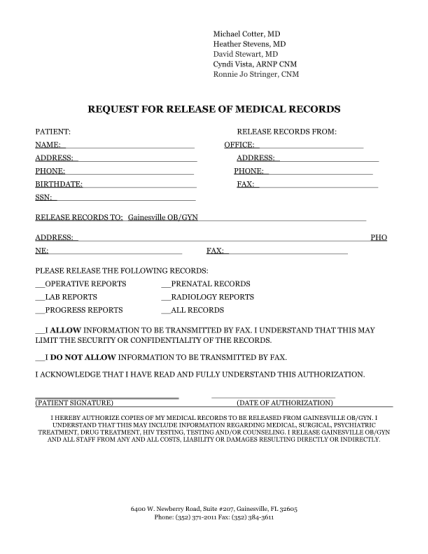
blank medical records release form
Medical records release/request form (please complete all blanks) we suggest that you keep a set of your medical record you requested. we shall send your medical record to you unless you want us to send it to your doctor, by mail or by fax (please...
FILL NOW