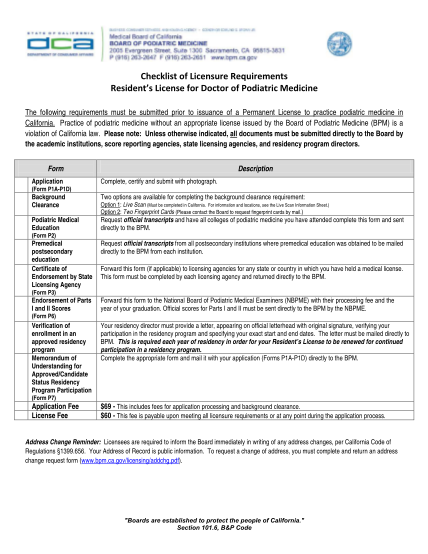
Board of Podiatric Medicine - Checklist of Licensure Requirements - Residents License for Doctor of Podiatric Medicine Board of Podiatric Medicine - Checklist of Licensure Requirements - Residents License for Doctor of Podiatric Medicine -
Checklist of licensure requirements residents license for doctor of podiatric medicine the following requirements must be submitted prior to issuance of a permanent license to practice podiatric medicine in california. practice of podiatric...
FILL NOW